Bone Cement Cure Testing, Simplified
Knee arthroplasty, or total knee replacement, is a common surgical procedure in which bone cement (polymethylmerthacalate or PMMA) is utilized to secure a total knee implant to the patient’s bone. The cement starts as a powder and a liquid that are mixed in the operating room. The cement is applied in a semi-liquid state between the bone and implant and then cures into a fully solid form, grouting the implant to the bone. Avoiding joint motion before the cement is fully cured is crucial, as any movement could lead to incomplete fixation of the implant, resulting in revision surgery.
The current state-of-the-art method to determine cement cure during surgery involves applying wet cement to the surgical site and then placing a separate ball of cement on a nearby table. When the surgeon determines that the ball of cement on the table has cured, the assumption is that the cement at the surgical site is also cured. Considering that the cost of a total knee replacement revision in the United States typically ranges from $35,000 to $50,000 or more, any early knee movement leading to the need for a revision surgery can result in substantial expenses for the patient.

Initial Development
Dr. Daniel Funk set out to develop a novel device to determine cement cure beneath the tibial tray of a total knee arthroplasty. By accurately alerting the surgeon to proper cement cure, it would be possible to decrease the incidence of knee motion before curing, lowering the risk of incomplete fixation of the implant.
Dr. Funk approached Priority Designs with a benchtop device he created to assess cement cure by measuring cement temperature. In a peer-reviewed published article written by Dr. Funk in the
Journal of Orthopaedic Surgery and Research, it was proven that a mathematical algorithm based on temperature could accurately determine cement cure. However, the device created by Dr. Funk only collected data, with interpretation done manually in Excel. Additionally, the device’s probe needed to be redesigned with a biocompatible material that could be inserted and removed from the cured cement.
Dr. Funk’s goal was to refine the device for clinical use by outlining a regulatory strategy, aquiring design inputs for biocompatibility, integrating a user interface, planning verification and validation, mitigating risks, and ensuring manufacturability.

Subject Matter Expert Interviews
To assure the development team was focused on user needs from the onset, our research team conducted interviews with licensed Orthopedic surgeons who had published peer-reviewed articles on cementing techniques in total joint arthroplasty. These individuals shared insights into current cement curing techniques in total knee arthroplasty, discussed challenges associated with monitoring cure time, and provided their professional opinions on the feasibility of Dr. Funk’s prototype. This information provided valuable guidance throughout the remainder of the development process.
Regulatory Strategy and Hazard Analysis
The first step of the development process was to determine a regulatory evaluation and conduct a preliminary hazard analysis. Our regulatory partner, CMD MedTech, helped search for potential predicates (similar devices) for FDA submission and classification. The result of this work was a written risk management document and a clear pathway to FDA submission.
Our team met routinely with Dr. Funk to discuss additional requirements and concerns, such as the device size and conformation, operating room function, and necessary alert notifications.
Our biomedical engineers understood that utilizing coded software would complicate the regulatory process, thus choosing to avoid software all together. As a result, we were able to develop a unique, patentable, fully analog circuit design. Refinements of the device included considerations such as ensuring it could fit comfortably in a user’s hand, guaranteeing the probe housing was large enough for easy removal, and establishing its placement within a surgical setting.
Mitigating Risks
The primary challenge was to ensure that the probe did not become incarcerated in the cement and that it could be extracted using tools readily accessible during knee replacement surgery without compromising the integrity of the cement bond.

Our engineering team generated a test fixture using our our Mark-10 machine, designed for measuring pull strength, to extract various sheets of material out of cured cement. Results were analyzed with the intention to meet current human factors and ergonomic benchmarks for hand strength. Our results showed that a shearing (a twisting motion) resulted in easier removal. We then identified a coating used in comparable medical devices, that come into contact with the body beneath the skin, such as trocars. This coating was chosen to address potential biocompatibility concerns and could also contribute to reduce the necessary force needed for removal.

An important design element to consider was the ability to sterilize the device for intraoperative use. We determined the device needed to be designed for EtO (Ethylene Oxide) “Gas” Sterilization rather than using high-heat steam, due to the electronics in the device. The appropriate materials and design elements were specified to assure proper sterilization.
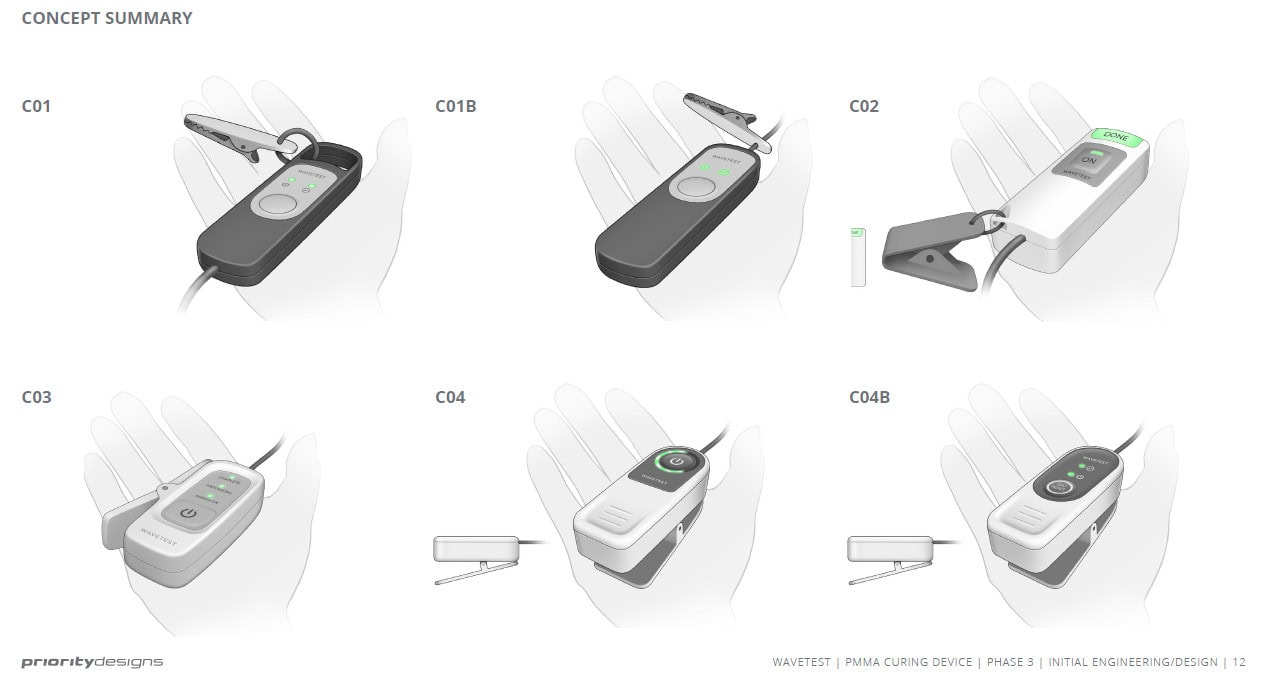
Engineering & Industrial Design
Our industrial design and biomedical engineering teams met to review the device requirements and insights from previous phases to develop a variety of potential device configurations. Following a client review of the proposed configurations, Dr. Funk ultimately chose the final direction for the device. From there, we created the CAD for a breadboard model to verify functionality.

Our mechanical engineering, industrial design, and electrical engineering teams collaborated to refine the board shape and adjust the size of the device. This iterative process continued until a model was achieved that could accommodate the required electronic components while aligning with previously determined functional requirements.

After finalizing the design elements, the CAD was handed off to our prototyping team where a functional prototype was created. As our electrical engineering team built the PCB (printed circuit board), our prototyping specialists printed the fob on our HP 3D printer using Nylon 12 polymer, then sanded and painted it to finish. The probe was urethane molded using stainless steel hypodermic tubing and a thermocouple insert and was assembled with custom parts acquired from approved vendors.



Functional Testing
Our engineering team created a testing configuration comprised of a block of closed-cell polyurethane foam (a material resembling bone that is used for surgical training and testing), a machined piece of aluminum emulating a tibial tray implant, and a system designed to submerge a significant portion of the bone-substitute material in circulating water at body temperature.


The experiment was designed to compare the device’s assessment of cement cure with the current standard procedure of allowing excess cement to cure naturally. Utilizing the ASTM’s (American Society for Testing and Materials) standard formula for cured bone cement, we established the cure time for both cement conditions. The results validated that our device consistently indicated cure at or shortly after the ASTM formula for the knee simulation cement, proving the device worked as intended. The tabletop sample cured at different times depending on humidity and temperature of the room, proving our device was more accurate compared to the current practices.


FDA Compliance
In collaboration with our regulatory partner, CMD MedTech, we documented each stage within our ISO 13485 compliant quality system and engaged in pre-submission discussions with the FDA to address specific concerns related to device classification and testing requirements.

Solution
The result was a handheld market-ready orthopedic instrument. Initially presented to us during its investigational stage, the device lacked essential considerations and documentation required for marketability. In partnership with Dr. Funk, we developed a hazard analysis and risk management system and provided initial contact with the FDA. Leveraging our expertise and partnerships, we provided design inputs focusing on usability and sterilization. A significant modification involved transitioning the electronic sensing device from digital to analog, a unique feature prompting Dr. Funk to pursue a patent. Finally, we combined the expertise of our in-house design, engineering, prototyping teams to supply Dr. Funk with pre-production prototypes for presentation to perspective partners.





